Summary EMDR 2.0
Ad de Jongh & Suzy Matthijssen
Introduction
The Evolution of Trauma Therapy
The field of trauma therapy has seen remarkable advances in recent decades, with EMDR (Eye Movement Desensitization and Reprocessing) therapy standing out as a transformative approach. Developed in the late 1980s by Francine Shapiro, EMDR therapy was initially met with skepticism, often dismissed as a pseudoscientific technique. Over time, empirical research solidified its reputation, particularly in its ability to address post-traumatic stress disorder (PTSD; De Jongh et al., 2024). However, as with any pioneering methodology, EMDR faced the need for refinement.
EMDR 2.0
EMDR 2.0 is an evolution of the original model, incorporating insights from cognitive psychology, neuroscience, and memory reprocessing research (De Jongh et al., 2024; Matthijssen et al., 2021). This enhanced version offers a more structured, efficient, and theoretically grounded approach to trauma therapy. By integrating working memory theory (Baddeley et al., 2012) and reconsolidation mechanisms, EMDR 2.0 deepens our understanding of how traumatic memories are processed and provides clinicians with more effective tools for their work.
This paper offers a comprehensive exploration of EMDR 2.0, tracing its historical roots, unpacking its theoretical foundations, and guiding practitioners through its practical application. We will also reflect on its broader implications for psychotherapy.
Historical Foundations
From controversy to validation
EMDR’s journey began with Shapiro’s serendipitous discovery that specific eye movements appeared to reduce the distress associated with traumatic memories. Initially, the therapy faced sharp criticism dismissing it as reminiscent of "mesmerism," a discredited 18th-century practice involving magnetic fields and theatrical healing rituals. McNally's critique highlighted the lack of a robust scientific framework supporting EMDR’s efficacy. At the time, the role of bilateral stimulation (BLS) remained unclear, and some critics dismissed the eye movements as unnecessary theatrics. The absence of a coherent theoretical model further fueled skepticism, with EMDR dismissed by many as an elaborate placebo. However, the late 1990s and early 2000s marked a turning point. Pioneering studies began to demonstrate the physiological and psychological changes induced by EMDR, particularly its ability to reduce the vividness and emotional intensity of traumatic memories. Research into working memory (WM) taxation shed light on the mechanisms underlying its success. By 2008, studies confirmed that engaging in WM taxing tasks during memory recall could diminish the emotional impact of distressing memories. These insights laid the foundation for EMDR 2.0, a refined protocol that bridges theory and practice.
Theoretical Foundations of EMDR 2.0
EMDR 2.0 builds on two core theories: Working Memory Theory and Reconsolidation Theory. Together, these frameworks provide a cohesive understanding of how traumatic memories are accessed, and processed according to Shapiro’s Adaptive Information Processing (AIP) model.
Working Memory Theory
Working memory is the cognitive system responsible for holding and manipulating information in the present moment (Wadji et al., 2022). However, this system has limited capacity, and tasks that demand simultaneous attention can strain it. The WM taxation hypothesis posits that dual-tasking during memory recall, so holding a memory in mind while performing another cognitively demanding activity, creates interference that reduces the memory's vividness and emotional charge (De Voogt & Phelps, 2020) . In the context of EMDR, tasks such as bilateral eye movements or alternating tactile stimulation compete for cognitive resources, weakening the grip of traumatic memories. Research highlights several key principles:
- Task Speed and Complexity: Faster eye movements and more complex tasks (e.g., backward counting or spelling) create greater WM interference, enhancing therapeutic effects.
- Task Modality: While eye movements are effective, other forms of dual-tasking, such as auditory or kinaesthetic activities, can achieve similar outcomes, as does modality-specific taxation that matches the emotionality of a memory.
- Emotional Relevance: The impact of WM taxation is most pronounced when applied to emotionally charged memories, underscoring the importance of activating distressing material during therapy.
Reconsolidation Theory
Memory reconsolidation occurs when a memory is retrieved, temporarily destabilizing its neural representation. During this window of plasticity, the memory becomes susceptible to modification. By pairing memory recall with WM taxation or other interventions, EMDR 2.0 facilitates the creation of a less distressing, updated version of the memory, which is then re-stored. Together, working memory theory and reconsolidation theory provide a robust scientific basis for EMDR 2.0, explaining its ability to induce lasting change in trauma-related memory reprocessing.
Core Components of EMDR 2.0
While EMDR 2.0 retains the eight-phase structure of the standard protocol, it introduces significant refinements to optimize client outcomes. At its core, EMDR 2.0 focuses on three pillars: motivation, activation, and desensitization.
- Motivation
Engaging clients in the therapeutic process is critical to the success of EMDR 2.0. The motivational phase involves educating clients about the therapy's mechanisms, setting clear expectations, and fostering collaboration. This phase often includes:
- Explaining the concept of WM taxation and how it helps reduce memory distress.
- Using accessible metaphors, such as a “competition” between the memory and the dual-tasking activity, to demystify the process.
- Encouraging clients to actively participate (acting as a “co-therapist”) despite potential initial discomfort.
Motivation serves not only to empower clients but also creates rapport with the therapist, thereby laying a foundation of trust and engagement that is essential for effective therapy.
- Activation
Effective activation is a cornerstone of EMDR 2.0. This phase involves accessing and vividly recalling the target memory, ensuring it is fully "online" for reprocessing. Techniques used to activate specific memories include:
- Guided Visualization: Helping clients focus and attune to the most distressing aspects of the memory to ensure thorough activation.
- Sensory Triggers: Engaging clients’ senses by exposing them to Visual (imagery; photos), Auditory (sounds), Kinaesthetic (tactile, e.g. adopting postures), Olfactory (smells) and Gustatory (taste) sensations (VAKOG) associated with the memory
For instance, a client revisiting a memory of childhood bullying might be guided to confront the faces of the bullies (e.g., through Facebook pages), as well as listen to sounds and physical sensations experienced during the event. Modality-specific taxation can also be used to combat aspects of an image, when the memory is stuck on a sensory fragment. For example, smelling coffee while thinking about the smell of smoke from the fire, or holding an ice pack or cold washcloth while thinking about the heat from the fire.
- Desensitization
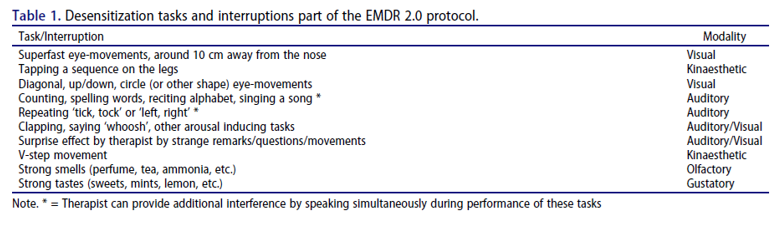
The Desensitization phase employs dual-tasking to reduce the memory's emotional impact. Unlike the original EMDR protocol, EMDR 2.0 emphasizes a broader range of tasks and adaptive strategies:
- Eye movements: e.g. lateral and vertical eye movements, as well as circular or multidirectional movements, tailored to client preferences.
- Cognitive Distractions: e.g. asking clients to count backward by threes, spell words backward, or name objects within a specific category (e.g., animals or vegetables).
- Modality specific taxing: e.g. tailoring interventions to the sensory modality of the memory (e.g., auditory tasks for sound-based memories) strengthens the connection between the task and the memory, increasing its efficacy.
- Surprise effects: e.g. introducing unexpected elements, such as humorous prompts or rapid task changes, disrupts memory reprocessing. This technique, known as "disruption by surprise," accelerates desensitization by increasing clients’ arousal level to help them shift their perspective.
- Tactile Tasks: e.g. alternating tapping patterns, or V-shape movement patterns often combined with additional cognitive challenges like eye movements.
Each task is designed to tax WM, creating a cognitive overload that disrupts the memory's vividness and emotional intensity (see Table 1).
In their extensive literature review on PTSD, Burback et al (2023) describe EMDR 2.0 as follows: ‘EMDR 2.0 is a modification of EMDR, which emphasizes motivational techniques to reduce avoidance, optimal activation of the trauma memory network, and multiple, often simultaneous, dual attention tasks to vigorously tax working memory while the memory is desensitized [621]. The patient is asked to place the traumatic event into working memory in all its detail, with psychoeducation regarding the proposed working mechanism of the treatment. Activating the traumatic memory takes place by focusing on the sensory aspects to optimize the arousal level. Arousal may also be altered by, for instance, adding surprising comments or unexpected sounds or gestures. Different memory-taxing tasks are at the disposal of the therapist, in various sensory modalities (e.g., visual, auditory, olfactory, gustatory), during a therapy session; some of these may use trauma reminders if enhancement of arousal is desired. The distractive task is often matched with the predominant sensory modality of the trauma memory, as there are some indications that this has a larger impact [622, 623]. EMDR 2.0 may also incorporate other imaginal or somatic elements, such as modifying posture or using movement. EMDR 2.0 also includes specific techniques to titrate the experience and counter dissociation or extreme avoidance.’
Research results on which EMDR 2.0 is based
- The more strongly the memory is activated, the better the effect of EMDR therapy (Van Veen, Engelhard & van den Hout, 2016)
- More arousal appears to have a stronger desensitizing effect, both with regard to the memory itself (Van den Hout et al., 2014) and in general (Littel et al., 2017)
- The greater the working memory load, the greater the desensitizing effect (De Jongh et al., 2013; van Veen et al., 2015; Littel & Van Schie, 2019)
- Modality-specific loading can, in certain cases, have an additional effect (Matthijssen et al., 2017; Matthijssen et al., 2018)
- Unexpected (surprise) effects can hinder the reconsolidation of the memory interrupt (Sinclair & Barensel, 2018; Matthijssen et al., 2019).
Innovative Techniques in EMDR 2.0
EMDR 2.0 introduces six advanced techniques to enhance therapeutic outcomes and address a wider range of clinical needs.
- Blind to therapist
- Titration techniques
- EMD bomb
- Flash 1.0
- Flashforwards
- Mental Video Check
Interweaves
Interweaves are targeted interventions used to address blocks in reprocessing. For people with significant trauma histories, interweaves are extremely suitable to bring about a breakthrough, especially in people with relational injuries where a lack of self-compassion or self-hatred are predominant.
Research supporting the efficacy of EMDR 2.0
The efficacy of EMDR 2.0 is supported by single case studies (e.g., De Jongh & Hafkemeijer, 2024; Matthijssen & Menses., 2024), a randomized experimental study (Matthijssen et al., 2021) and by clinical outcome studies, both uncontrolled studies among veterans (Reij et al., 2025), adolescents with PTSD (Rentinck et al., 2025) and adults with PTSD (Van der Linde et al., 2023; Van Woudenberg et al., 2023; Matthijssen et al., 2024), borderline personality disorder (Kolthof et al., 2022), by randomized outcome studies in the field of PTSD (Alting van Geusau et al., in preparation; Yassar et al., 2024 & 2025) and personality disorders with and without PTSD (Hofman et al., submitted for publication). Furthermore, there is scientific support for the application of EMDR 2.0 using telehealth (Ellenbroek et al., 2024; Yassar et al., 2024 & 2025) and group practice (Matthijssen & Menses, 2024; Yassar et al., 2024 & 2025). See the attachment with a description of all 12 studies.
The Future of EMDR 2.0
EMDR 2.0 represents a leap forward in EMDR therapy, integrating scientific advancements with practical innovations. Its emphasis on working memory taxation, tailored interventions, and client engagement offers a powerful framework for addressing a range of psychological conditions. As ongoing research continues to validate its efficacy, EMDR 2.0 is poised to play an increasingly central role in the treatment of trauma and beyond. For clinicians, mastering this approach provides not only a deeper understanding of trauma-focused reprocessing but also a transformative tool for fostering lasting healing.
References
In their extensive literature review on PTSD, Burback et al (2023) describe EMDR 2.0 as follows:
‘EMDR 2.0 is a modification of EMDR, which emphasizes motivational techniques to reduce avoidance, optimal activation of the trauma memory network, and multiple, often simultaneous, dual attention tasks to vigorously tax working memory while the memory is desensitized [621]. The patient is asked to place the traumatic event into working memory in all its detail, with psychoeducation regarding the proposed working mechanism of the treatment. Activating the traumatic memory takes place by focusing on the sensory aspects to optimize the arousal level. Arousal may also be altered by, for instance, adding surprising comments or unexpected sounds or gestures. Different memory-taxing tasks are at the disposal of the therapist, in various sensory modalities (e.g., visual, auditory, olfactory, gustatory), during a therapy session; some of these may use trauma reminders if enhancement of arousal is desired. The distractive task is often matched with the predominant sensory modality of the trauma memory, as there are some indications that this has a larger impact [622, 623]. EMDR 2.0 may also incorporate other imaginal or somatic elements, such as modifying posture or using movement. EMDR 2.0 also includes specific techniques to titrate the experience and counter dissociation or extreme avoidance.’
References
Alting van Geusau, V.V.P., de Jongh, A., Nuijs, M.D., Brouwers, T.C., Moerbeek, M. & Matthijssen, S.J.M.A. (2023) The effectiveness, efficiency, and acceptability of EMDR vs. EMDR 2.0 vs. the Flash technique in the treatment of patients with PTSD: study protocol for the ENHANCE randomized controlled trial. Frontiers in Psychiatry, 14, 1278052. https://doi.org/10.3389/fpsyt.2023.1278052
Alting van Geusau, V.V.P., Nuijs, M.D., De Jongh, A., Moerbeek, M. & Matthijssen< S.M.J.A. (2025) The relationship between changes in emotional intensity and treatment outcome in PTSD patients in EMDR therapy. European Journal of Psychotraumatology, 16:1, 2536973. https://doi.org/10.1080/20008066.2025.2536973
Baddeley, A.D. (2012). Working memory: theories, models, and controversies. Annual Review of Psychology, 63, 12.1-12.29.
Burback, L., Brémault-Phillips, S., Nijdam, M.J., McFarlane, A.C., & Vermetten, E. (2023). Treatment of Posttraumatic Stress Disorder: A State-of-the-art Review. Current Neuropharmacology, 22, 557 - 635.
De Jongh A., Ernst, R, Marques, L. & Hornsveld, H. (2013). The impact of eye movements and tones on disturbing memories of patients with PTSD and other mental disorders. Journal of Behavior Therapy and Experimental Psychiatry, 44, 447-483.
De Jongh, A., De Roos, C., El-Leithy, S. (2024). State of the science: Eye movement desensitization and reprocessing (EMDR) therapy. Journal of Traumatic Stress, 37, 2, 205–216. https://doi.org/10.1002/jts.23012
De Jongh, A., & Hafkemeijer, L.C.S. (2024). Trauma‐focused treatment of a client with Complex PTSD and comorbid pathology using EMDR. Journal of Clinical Psychology, 80, 824–835. https://doi.org/10.1002/jclp.23521
De Voogd, L. D., & Phelps, E. A. (2020). A cognitively demandin working memory intervention enhances extinction. Scientific Reports, 10(1), Article 7020. https://doi.org/10.1038/s41598-020-63811-0
Ellenbroek, N., Nuijs, M. D., & Matthijssen, S. J. (2024). The effectiveness of a remote intensive trauma-focused treatment programme for PTSD. European Journal of Psychotraumatology, 15(1), 2408960. https://doi.org/10.1080/20008066.2024.2408960
Hofman, S., Hafkemeijer, L.C.S., De Jongh, Slotema, K. (in press). Effectiveness of EMDR therapy on symptoms and diagnostic status of personality disorders: a multicenter randomized controlled trial. JAMA Psychiatry Network
Kolthof, K.A., Voorendonk, E.M., Van Minnen, A., De Jongh, A. (2022). Effects of intensive trauma-focused treatment of individuals with both post-traumatic stress disorder and borderline personality disorder. European Journal of Psychotraumatology, 13:2, 2143076. https://doi.org/10.1080/20008066.2022.2143076
Littel, M. & van Schie, K. (2019). No evidence for the inverted U-Curve: More demanding dual tasks cause stronger aversive memory degradation Journal of Behavior Therapy and Experimental Psychiatry, 65, 101484.
Matthijssen,, S.J.M.A., Brouwers,, T.C., van Roozendaal, C., Vuister T.C.M., De Jongh, A. (2021) The effect of EMDR versus EMDR 2.0 on emotionality and vividness of aversive memories in a non-clinical sample. European Journal of Psychotraumatology, 12 (1), 1956793, https://doi.org//10.1080/20008198.2021.1956793
Matthijssen, S. J., & Menses, S. D. (2024). Case report: Intensive online trauma treatment combining prolonged exposure and EMDR 2.0 in a patient with severe and chronic PTSD. Frontiers in Psychiatry, 15, 1370358.
Matthijssen, S. J., Menses, S. D., & Huisman-van Dijk, H. M. (2024). The effects of an intensive outpatient treatment for PTSD. European Journal of Psychotraumatology,15(1), https://doi.org/10.1080/20008066.2024.2341548
Matthijssen, S. J. M. A., Heitland, I., Verhoeven, L. C., & Van den Hout, M. A. (2019). Reducing the emotionality of auditory hallucination memories in patients suffering from auditory hallucinations. Frontiers in Psychiatry, 10, 637. https://doi.org/10.3389/fpsyt.2019.00637
Reij, K.M., De Jongh, A., Swens, E.P., Voorendonk, E.M. (2025). PTSD Symptoms change in response to a brief intensive trauma-focused treatment programme in non-veterans and veterans with war-related PTSD. European Journal of Psychotraumatology, 16, 1, https://doi.org/10.1080/20008066.2025.2511571
Rentinck, E.M., van Mourik, R., De Jongh & Matthijssen, S.J.M.A (2025). Effectiveness of an intensive outpatient treatment programme combining prolonged exposure and EMDR therapy for adolescents and young adults with PTSD in a naturalistic setting. European Journal of Psychotraumatology. 16:1, 2451478. https://doi.org/10.1080/20008066.2025.2451478
Sinclair, A. H., & Barense, M. D. (2018). Surprise and destabilize: Prediction error influences episodic memory reconsolidation. Learning & Memory, 25(8), 369-381. https://doi.org/10.1101/lm.046912.117
Van den Hout, M. A., Eidhof, M. B., Verboom, J., Littel, M., & Engelhard, I. M. (2014). Blurring of emotional and nonemotional memories by taxing working memory during recall. Cognition and Emotion, 28, 717–727.
Van der Linde, R.P.A., Huntjens, R.J.C., Bachrach, N., Rijkeboer, M.M., De Jongh, A. & Van Minnen, A. (2023). The role of dissociation-related beliefs about memory in trauma-focused treatment. European Journal of Psychotraumatology, 14:2, 2265182. https://doi.org/10.1080/20008066.2023.2265182
van Veen, S.C., Engelhard, I.M., & van den Hout, M.A. (2016). The effects of eye movements on emotional memories: using an objective measure of cognitive load. European Journal of Psychotraumatology, 7.
Van Veen, S.C., Schie, K. van, Wijngaards-de Meij, L.D.N.V., Littel, M., Engelhard, I.M. & Hout, M.A. van den (2015). Speed matters: relationship between speed of eye movements and modification of aversive autobiographical memories. Frontiers in Psychiatry, 6, 2-9.
Van Woudenberg, C., Voorendonk, E.M., Tunissen, B., van Beek. V.H.F., Rozendael, L., Van Minnen, A. & De Jongh, A. (2023). The impact of intensive trauma-focused treatment on sexual functioning in individuals with PTSD. Frontiers in Psychology, 14:1191916. https://doi.org/10.3389/fpsyg.2023.1191916
Yaşar, A.B., Kavakçı, Ö., Çiftçi, Z.Z., Tunca, G.A., Uygun, E., Gündoğmuş, İ., Kubilay, D., Aksöz, Y., Deveci, H., & Konuk, E. (2023). The Effectiveness of Online EMDR 2.0 Group Protocol on Posttraumatic Stress Disorder Symptoms, Depression, Anxiety, and Stress in Individuals Who Have Experienced a Traffic Accident: A Preliminary Study. Journal of EMDR Practice and Research, 17, 171-184.
Yasar, A.B., Gundogmus ˙I., Kubilay, D., Alban Tunca, G., Uygun, E., Zat Çiftçi, Z. & Kavakcı, Ö. (2025). The effectiveness of online Eye Movement Desensitization and Reprocessing 2.0 Group Protocol on post-traumatic stress disorders symptoms, depression, anxiety, and stress in individuals who have experienced a traffic accident: a randomized-controlled study. Frontiers in Psychiatry, 16:1452206. doi: 10.3389/fpsyt.2025.1452206
Attachments: Studies supporting the efficacy of EMDR 2.0
- The effect of EMDR versus EMDR 2.0 on emotionality and vividness of aversive memories in a non-clinical sample (Matthijssen et al., 2021)
In a randomized controlled study 62 non-clinical participants with disturbing autobiographical memories were treated with either standard EMDR therapy or the adapted EMDR 2.0 protocol. Both interventions led to significant and lasting reductions in emotionality and vividness of the memories, measured immediately after treatment and at one- and four-week follow-ups. However, no significant differences were found between the two groups in terms of efficacy. Regarding efficiency, participants in the EMDR 2.0 condition required significantly fewer desensitization sets than those in the standard EMDR group to achieve the same therapeutic effects. Despite this, session duration was comparable between the two groups. Hence, EMDR 2.0 proved equally effective but potentially more efficient than standard EMDR, as it requires fewer working memory taxation sets. Further research in clinical populations is recommended to explore its added value.
- The role of dissociation-related beliefs about memory in trauma-focused treatment (Van der Linde et al., 2023)
This study investigated whether dissociation-related beliefs about memory (e.g., beliefs that traumatic memories are too overwhelming or dangerous to access) affect treatment outcomes in individuals undergoing prolonged exposure and EMDR 2.0. A sample of 71 patients with PTSD completed self-report measures before and after treatment, including assessments of dissociation-related beliefs. The results showed that stronger dissociation-related beliefs at baseline were significantly associated with smaller reductions in PTSD symptoms after treatment. These beliefs predicted treatment outcome beyond general dissociative symptoms and baseline PTSD severity. Importantly, the beliefs themselves decreased significantly during treatment, and reductions in these beliefs were associated with greater symptom improvement. Hence, addressing and challenging these beliefs may enhance the effectiveness of TFT.
- Effects of intensive trauma-focused treatment of individuals with both post-traumatic stress disorder and borderline personality disorder (Kolthof et al., 2022)
This study examined the effectiveness and safety of intensive trauma-focused treatment for individuals diagnosed with both PTSD and borderline personality pathology. A total of 47 participants underwent an eight-day treatment program consisting of EMDR 2.0 prolonged exposure, psychoeducation, and physical activities, all delivered without a preceding stabilization phase. The findings demonstrated significant reductions in both PTSD and borderline symptoms immediately post-treatment, with these improvements maintained at the three-month follow-up. No symptom deterioration was observed, and the dropout rate was low (6.4%). Furthermore, 51.1% of participants no longer met diagnostic criteria for PTSD following treatment. The results showed that intensive trauma-focused treatment without prior stabilization was both effective and safe for individuals with comorbid PTSD and borderline personality features. These findings challenge the commonly held belief that stabilization is a necessary prerequisite in this population.
- The impact of intensive trauma-focused treatment on sexual functioning in individuals with PTSD (Van Woudenberg et al., 2023).
This study investigated whether an intensive trauma-focused treatment program consisting of daily EMDR 2.0 and prolonged exposure therapy could improve sexual functioning in individuals with PTSD, a symptom domain often neglected in trauma treatment research. A total of 227 participants completed this eight-day program, supported by physical activity and psychoeducation, with no preceding stabilization phase. The results showed a significant reduction in PTSD symptoms, as well as a moderate but significant improvement in overall sexual functioning from pre- to post-treatment. These improvements were maintained at the six-month follow-up. Notably, changes in sexual functioning were significantly associated with reductions in PTSD symptoms, suggesting a meaningful clinical relationship. These findings highlight the relevance of addressing sexual health in trauma recovery and suggest that such improvements can occur without specific interventions targeting sexuality.
- The Effectiveness of Online EMDR 2.0 Group Protocol on Posttraumatic Stress Disorder Symptoms, Depression, Anxiety, and Stress in Individuals Who Have Experienced a Traffic Accident: A Preliminary Study (Yassar et al., 2023).
This pilot study examined the feasibility and effectiveness of the Online EMDR 2.0 Group Protocol for adults with PTSD symptoms following the 2023 earthquakes in Turkey. A total of 33 participants received four 90-minute online group EMDR 2.0 sessions over one week. The intervention was designed for rapid deployment in the aftermath of collective trauma, using a fully remote, video-conferencing format. Participants reported significant reductions in PTSD symptoms, distress, and functional impairment immediately after the intervention. These improvements were maintained at one-month follow-up. Nearly half of the participants no longer met the threshold for probable PTSD post-treatment. The protocol was well received, with high attendance, no adverse effects, and strong participant satisfaction. This study offers promising evidence that brief, remote EMDR 2.0 group interventions may be a practical and effective option for early response in disaster settings. It highlights the potential for scalable, trauma-focused care, even in low-resource and high-stress contexts.
- Case report: Intensive online trauma treatment combining prolonged exposure and EMDR 2.0 in a patient with severe and chronic PTSD (Matthijssen & Menses, 2024)
A woman with chronic and severe PTSD, stemming from a history of complex childhood trauma, underwent an innovative six-day online treatment program combining Prolonged Exposure (PE) and EMDR 2.0. Each day included structured components: PE, physical exercise, EMDR 2.0 using a digital tool, and psychoeducation. Despite significant comorbidity—including depression, panic disorder, and personality disorder traits—she completed the program without any adverse effects. The results were striking: all PTSD symptoms remitted and remained absent at six-month follow-up. Additionally, her depressive and general psychiatric symptoms dropped from severe to minimal levels. This case demonstrates the feasibility and potential effectiveness of fully remote, intensive trauma treatment, even in patients with complex clinical presentations. It opens new doors for care delivery in situations where in-person therapy is not possible or preferred.
- The effects of an intensive outpatient treatment for PTSD (Matthijssen et al., 2024)
This study evaluated the outcomes of an intensive, trauma-focused outpatient treatment program for adults with PTSD in routine clinical care. A total of 234 participants, many of whom had experienced multiple interpersonal traumas and had complex comorbidities, completed an eight-day treatment course. The program combined daily EMDR 2.0 and prolonged exposure therapy with physical activity and psychoeducation, without any preparatory stabilization phase. PTSD symptoms decreased significantly across the sample, with large effect sizes, and these improvements were maintained at three-month follow-up. Over half of the participants no longer met diagnostic criteria for PTSD after treatment. Importantly, the dropout rate was low, and no symptom worsening was observed, even among patients with a history of childhood trauma or personality disorders. These findings demonstrate that trauma-focused therapy can be delivered safely and effectively in an intensive, short-term format, even in real-world clinical settings and for complex cases.
- The effectiveness of a remote intensive trauma-focused treatment programme for PTSD (Ellenbroek et al., 2024)
This study evaluated the effectiveness of a fully remote, intensive trauma-focused treatment program for adults with PTSD, delivered entirely via videoconferencing. A total of 73 participants received daily sessions of Prolonged Exposure and EMDR 2.0, along with physical activity and psychoeducation, over the course of eight days. The program was modeled after established in-person intensive treatment formats but adapted for remote delivery, without any pre-treatment stabilization phase.
The outcomes were strong: participants showed large reductions in PTSD symptoms from pre- to post-treatment, and these improvements were maintained at three-month follow-up. Over 60% of participants no longer met diagnostic criteria for PTSD after treatment. The intervention was well tolerated, with low dropout rates and no symptom deterioration, even in individuals with complex trauma histories and comorbid conditions.
These findings suggest that intensive trauma-focused therapy that combines exposure and EMDR 2.0 therapy can be delivered safely and effectively online, offering a promising solution for clients unable or unwilling to access in-person care.
- Effectiveness of an intensive outpatient treatment programme combining prolonged exposure and EMDR therapy for adolescents and young adults with PTSD in a naturalistic setting (Rentinck et al., 2025).
This study assessed the effectiveness of an intensive trauma-focused outpatient treatment program for adolescents with PTSD, incorporating both prolonged exposure and EMDR 2.0 therapy over an eight-day period. The sample included 48 adolescents aged 12–18 years, many of whom had experienced multiple interpersonal traumas and presented with complex clinical profiles. The results showed large and statistically significant reductions in PTSD symptoms immediately following treatment, which were maintained at three-month follow-up. At post-treatment, 62.5% of participants no longer met diagnostic criteria for PTSD. Additionally, the treatment was well tolerated, with low dropout and no evidence of symptom worsening, even among those with high initial symptom severity or comorbidities. The results support the notion that intensive trauma-focused treatment combining prolonged exposure and EMDR 2.0 therapy is both feasible and highly effective for adolescents with PTSD, including those with complex trauma histories.
- PTSD Symptoms change in response to a brief intensive trauma-focused treatment programme in non-veterans and veterans with war-related PTSD (Reij et al., 2025).
This study evaluated the effectiveness of a brief intensive trauma-focused treatment programme with war-related PTSD, comparing outcomes between veterans and non-veterans. The treatment consisted of eight consecutive days of daily prolonged exposure and EMDR 2.0 therapy, combined with physical activity and psychoeducation. Results indicated significant reductions in PTSD symptoms for both groups, with large effect sizes observed post-treatment and at three-month follow-up. Although non-veterans showed slightly greater symptom reduction, veterans also demonstrated substantial clinical improvement. Importantly, symptom deterioration was rare, and treatment dropout was minimal. These findings support the feasibility of condensed therapeutic formats in this population, including those with complex trauma histories.
- The effectiveness of online Eye Movement Desensitization and Reprocessing 2.0 Group Protocol on post-traumatic stress disorders symptoms, depression, anxiety, and stress in individuals who have experienced a traffic accident: a randomized-controlled study (Yassar et al., 2025).
This study randomized controlled trial investigated whether EMDR 2.0can be delivered effectively in a group format and entirely online. In the study, 41 adults with PTSD symptoms related to a recent earthquake were randomly assigned to either an online EMDR 2.0 Group Protocol or a waitlist control condition. The group intervention consisted of four 90-minute online sessions delivered over one week. The results were promising: participants in the EMDR 2.0 group showed significantly greater reductions in PTSD symptoms compared to the control group, with large effect sizes. These gains were maintained at four-week follow-up. Notably, more than 60% of participants in the intervention group no longer met criteria for probable PTSD after treatment. The protocol was well tolerated, with high attendance and no adverse events. This study provides preliminary but encouraging evidence that brief, online group-based EMDR 2.0 can be an effective and scalable intervention in the aftermath of mass trauma. It opens up new possibilities for rapid, remote mental health support in disaster-affected regions.
- Effectiveness of EMDR therapy on symptoms and diagnostic status of personality disorders: a multicenter randomized controlled trial (Hofman et al., in press)
A recently completed multicenter randomized controlled trial investigated whether EMDR 2.0 therapy can reduce symptoms of personality disorders, even in the absence of PTSD. In this study, 159 individuals with a DSM-5 personality disorder diagnosis received ten EMDR 2.0 sessions over a period of five weeks. The results were striking in that participants in the EMDR 2.0 condition showed significantly greater reductions in symptom severity compared to those on a waiting list, and nearly half no longer met diagnostic criteria for a personality disorder at three-month follow-up. Improvements were also observed in personality functioning and emotion regulation, and these effects were consistent across different types of personality disorders, including borderline and avoidant personality disorder. Importantly, the treatment was well tolerated, with a low dropout rate and no adverse events. These findings suggest that trauma-focused EMDR 2.0 therapy may offer an effective and efficient short-term intervention for individuals with personality disorders, even when PTSD is not present. The study challenges the prevailing assumption that long-term, insight-oriented treatment is always necessary in this population, and opens the door to new, modular approaches to care.
- The relationship between changes in emotional intensity and treatment outcome in PTSD patients in EMDR therapy (Alting van Geusau et al., 2025)
This study examined whether changes in emotional intensity during EMDR therapy predicted treatment outcome in 125 patients with PTSD following multiple traumatization. The intensive program included six EMDR sessions, delivered using EMDR 2.0, which applies higher working memory load than standard EMDR. Results showed that greater reductions in emotional intensity (measured by Subjective Units of Disturbance, SUD) were significantly associated with stronger decreases in PTSD symptoms at four-week follow-up. The number of traumatic images fully desensitized to a SUD score of zero emerged as the strongest predictor of treatment success, while age, gender, and dissociative PTSD subtype were not predictive. These findings highlight the clinical importance of monitoring changes in emotional intensity during EMDR 2.0 as an indicator of therapeutic progress and outcome
